Dr Vally is requiring us to draft treatment plans for continuing treatment as the current prescription draws to a close (3 sessions or 3 weeks left). This is kind of a hassle for us, but it does make some sense. After the first round of treatment, and you are familiar with the patients injuries, you have good insight to help the doctor determine the massage treatment goals for the next round of treatment. This form gathers the information we need to draft the next treatment plan. (This is IN ADDITION to the final report which is due at the same time)
It is good for you to understand the process from here in case the patient asks.
With your input from this form we will generate a proposal for the next round of treatment
The doctor will review and sign it and send it to the adjuster for approval
The adjuster will approve it and send it back to the doctor who will then send it to us
We let the patient know within 2 business days of receiving it from the doctor.
While this new procedure is a hassle for us, it will be a benefit to the patient. With your timely submission of the form, the new treatment plan gets generated automatically and sent to the doctor on the next business day. This will doubtlessly take less time than if the doctors office had to prepare it themselves, and in turn, will shorten lapse times between plans.
There are two sections we need you to fill out to help determine the treatment goals:
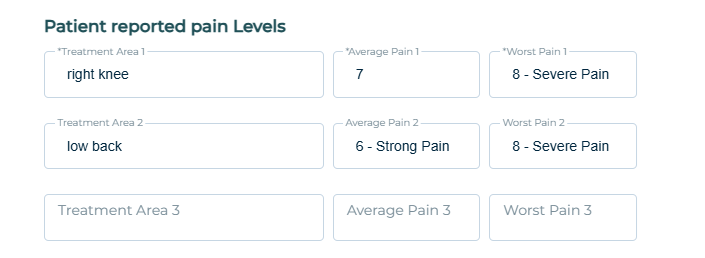
Record pain levels reported by the patient for their various diagnosed areas
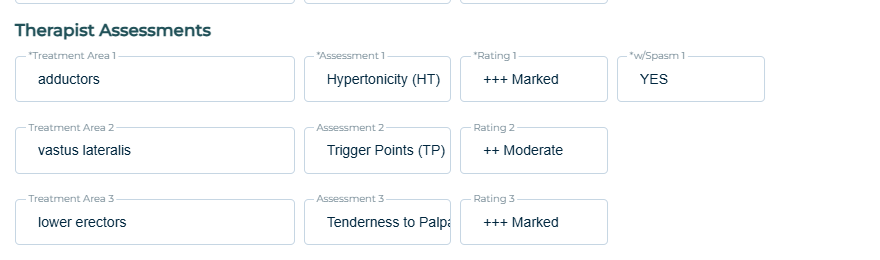
Report your assessment of hypertonicity, trigger points, and painfulness to palpation for the diagnosed areas
At least #1 you will have to ask the patient during your session. We suggest filling out the form in its entirety during the session and submitting it. It shouldn’t take more than a few minutes. Alternatively you can record the patients answers to their pain levels to enter in the form later.
The patient may have multiple diagnosis codes that cover multiple areas of the body. We don’t need answers for every single diagnosis code but we do need them for each area covered by the codes. For example consider this sample patient with the following diagnoses
M25.561: pain in right knee
S83.241D: Other tear of medial meniscus, current injury, right knee
M54.50: low back pain
M54.16: lumbar radiculopathy
While there are 4 diagnoses, they only cover 2 areas of the body:
right knee
low back.
In the first section of the form you need to ask the patient their pain levels each of these areas two areas. Ask them their average and worst pain over the past 7 days:
Then in the next section, you will report on your observations of the patient over the last few sessions. Ideally you will have at least one assessment for each area of the patient with diagnoses. You can list this as the general area, or as a muscle group, or as a specific muscle group. (Just make sure it makes sense and don’t talk about hypertonicity of a joint!)
Thank you so much. I know this is extra work for you but hopefully it will become routine and not take a lot of thought after the first few times. Doing this sort of thing is just one more thing that make the doctors love us and want to send us more patients.